

Vaginismus | Symptoms, Causes, and Effective Treatments
Introduction
Vaginismus is a common sexual disorder in women marked by involuntary tightening of the vaginal muscles when penetration is attempted. This can make intercourse painful or even impossible. Many women suffer in silence for years, assuming it is untreatable, but evidence-based therapies and psychosexual care can significantly improve or resolve it.
What is vaginismus
In this condition, the muscles around the vagina contract unconsciously and involuntarily, blocking comfortable penetration or causing severe pain.
Vaginismus can be
- Primary: present since the first attempts at intercourse.
- Secondary: develops after a period of pain free intercourse due to physical or psychological factors.
Signs and symptoms
Vaginismus is not defined by a single sign. It is a combination of physical symptoms and emotional reactions that together create the problem.

Physical symptoms
-
Severe pain with attempts at penetration
- Pain may feel burning, sharp, or like tearing.
- Pain is often intense enough to stop intercourse.
-
Involuntary vaginal muscle spasm
- The muscles around the vagina tighten without control.
- Many describe a feeling that the vagina is “closed” and nothing can enter.
-
Difficulty using tampons or during pelvic exams
- Inserting a tampon or speculum may be impossible.
- Sometimes only the tip can be inserted before pain or spasm starts.
-
A sensation of pressure or blockage
- Some patients describe an “invisible wall” at the vaginal entrance.
-
Vaginal dryness and irritation
- Avoidance and anxiety can reduce natural lubrication.
- This further increases pain and burning.
Psychological and emotional symptoms
-
Intense fear of penetration
- Anxiety can start even at the thought of intercourse.
- Fear itself can trigger stronger muscle contractions.
-
Avoidance of sexual activity
- Over time, a person may avoid sexual contact or even discussions about it.
- This can strain intimacy and the relationship.
-
Shame or guilt
- Some believe it reflects a personal weakness.
- These feelings lower self confidence and may lead to depression.
-
General body tension and stress
- During intimacy the whole body may tense, not just the pelvic floor.
- Sweating, palpitations, or shaking can occur.
Severity
Vaginismus ranges from mild penetration possible but painful to severe where even gentle touch triggers spasm.
- In primary vaginismus, penetration has never been possible.
- In secondary vaginismus, it appears after a period of normal intercourse for example after childbirth or infection.
Key point
Vaginismus is not only “pain with penetration.” It is pain plus fear and anxiety, which distinguishes it from problems like simple infection or dryness.
Causes and risk factors
The cause is often multifactorial, involving both psychological and physical contributors.
Psychological factors
- Fear of pain during first intercourse.
- Past sexual trauma or abuse.
- High anxiety or stress related to sex.
- Marital or communication difficulties.
Physical factors
- Recurrent vaginal or bladder infections.
- Marked vaginal dryness for example after menopause.
- Pelvic scarring or prior surgery.
- Rare neurologic or muscular disorders.
Diagnosis
- Detailed history of symptoms and medical background.
- Gentle pelvic exam by a clinician only if tolerated.
- Testing for infection or anatomic issues when indicated.
- Parallel psychosexual assessment.
Treatment of vaginismus
-
Education and counselling
- Clear, compassionate education about anatomy and the sexual response.
- Correcting myths for example penetration should not inherently be painful.
-
Psychotherapy and sex therapy
- Individual or couple based counselling.
- Cognitive behavioral therapy to reduce anxiety.
- Relaxation training and stress management.
-
Pelvic floor physical therapy
- Reverse Kegels relaxation focused pelvic floor work.
- Guidance from a pelvic health physiotherapist.
-
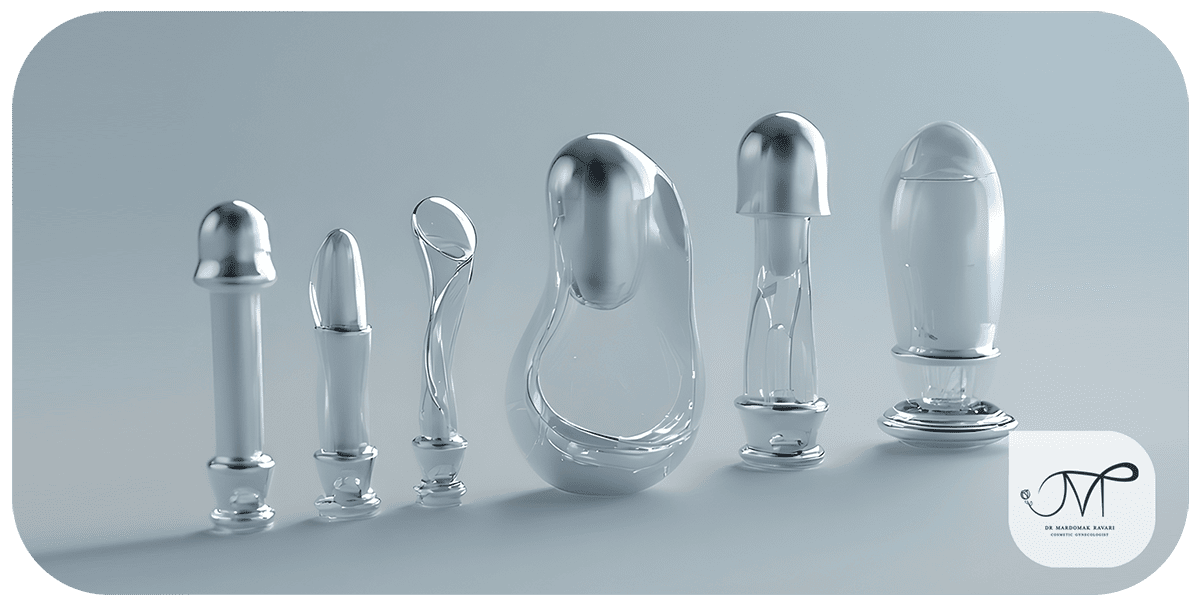
Vaginal dilators
- Graduated dilators inserted progressively.
- Help the body adapt to penetration and reduce spasm.
- Used along with relaxation and breathing techniques.
-
Psychiatry for severe cases
- Short term medications for significant anxiety or depression when appropriate.
-
Newer or adjunctive options
1. Botulinum toxin injections
- Temporarily relaxes hyperactive vaginal muscles and reduces involuntary spasm.
- Pros: relatively quick effect within days, useful for cases resistant to standard therapy, repeatable every 6 to 9 months if needed.
- Cons: cost, temporary benefit unless combined with therapy and exercises.
-
Vaginal laser or radiofrequency energy therapy
- Fractional CO2 laser or RF can treat dryness, atrophy, and tissue quality issues.
- Particularly helpful in secondary vaginismus linked to trauma, childbirth, surgery, or atrophic changes.
- Mechanism: collagen remodeling and improved blood flow leading to more elastic, comfortable tissue and less pain and spasm.
- Pros: noninvasive, minimal downtime, benefits may last 1 to 2 years.
-
PRP injections platelet rich plasma
- Autologous plasma rich in growth factors promotes tissue healing.
- In women with dryness, microtrauma, or scarring, PRP can improve tissue quality, reduce pain, and support sexual confidence.
- Pros: uses the patient’s own blood, generally low side effect profile.
-
Exosome based therapy
- Cell derived vesicles that modulate repair and inflammation.
- Early stage option in some centers for tissue regeneration in vaginismus with atrophy or scarring.
- Evidence is emerging and it is typically an adjunct to standard care.
-
Multimodal therapy
- Best outcomes often come from combining
- Counselling and sex therapy
- Pelvic floor therapy and dilators
- Plus botulinum toxin or laser PRP in resistant cases
Simple takeaway
Advanced options such as botulinum toxin, laser RF, PRP, and exosome based therapies are mainly for resistant vaginismus or cases with tissue problems like dryness or scarring. They are generally safe with low downtime but should be paired with psychosexual therapy and graded exercises for lasting results.
Prevention and self care
While vaginismus cannot always be fully prevented, lifestyle and relationship practices can lower risk and lessen severity.
-
Education and awareness
- Gaps in knowledge about anatomy and the sexual response foster fear and misconceptions.
- Reliable resources, premarital education, or sexual health workshops can reduce anxiety.
-
Healthy partner communication
- Honest conversations about fears and needs are protective.
- Unhurried intimacy and adequate foreplay ease muscle tension.
-
Anxiety and stress reduction
- General life stress can worsen vaginismus.
- Relaxation training, yoga, meditation, and deep breathing before intimacy help.
- Create a calm environment soft music, low light, a comfortable space to signal safety to the body.

-
Body care
- Use water based lubricants when dryness is present for example postpartum or in menopause.
- Treat vaginal or urinary infections promptly to prevent pain conditioned spasm.
- Avoid frequent douching or harsh soaps that trigger dryness and irritation.
-
Pelvic floor training especially reverse Kegels
- Focus on releasing rather than tightening the pelvic floor.
- Building awareness and voluntary relaxation reduces involuntary spasms.
- Learn with a women’s health physiotherapist when possible.
-
Psychological self care
- Accept that vaginismus is common and treatable.
- Avoid self blame or comparisons that raise anxiety.
- Seek trauma informed therapy when there is a history of abuse or deep seated fear.
-
Early action
- Do not wait if penetration is painful or spasm occurs. Early intervention is easier and faster.
- See a gynecologist and, when appropriate, a sex therapist.
Summary
Prevention and self care mean knowledge plus healthy communication plus calm mind and body plus tissue care plus relaxation focused pelvic floor training. Together they reduce onset and shorten recovery.
Clinical examples
Case 1
A 24 year old woman with pain and inability to achieve penetration since first attempts. After several counselling sessions and practice with small dilators, she achieved comfortable, complete intercourse.
Case 2
A 31 year old woman after a difficult childbirth developed pain and spasms with intercourse. Pelvic floor physiotherapy and relaxation training resolved her symptoms.
Case 3
A 40 year old woman with a history of sexual trauma developed secondary vaginismus. With trauma focused psychotherapy and partner support, she showed marked improvement over a year.
Conclusion
Vaginismus is a common but treatable sexual disorder, usually caused by a combination of psychological and physical factors.
Early diagnosis, consultation with a specialist, and gradual therapy can restore marital satisfaction and personal confidence.
The most important point is recognizing that this condition is both common and manageable—women should not live in silence with it.
In many women with vaginismus, pain during intercourse is the first and most distressing symptom.
This pain can worsen with vaginal dryness, especially during menopause.
Step-by-step treatment includes education, relaxation techniques, and pelvic floor physiotherapy.
Performing regular Kegel exercises, especially the relaxation or “reverse Kegel” version, helps reduce muscle spasm and gradually restore comfortable penetration.
Combining sexual education, psychotherapy, vaginal dilator training, and, in selected cases, modern interventions such as laser therapy or botulinum toxin (Botox) provides the best results.
Together, these methods improve intimacy, rebuild confidence, and help women regain control over their bodies and relationships.
Similar Articles

Pain or spasm with penetration?
Fill out the consultation form now and our assistant will contact you shortly.
 FAQ
FAQ
No comments have been posted.
Your email address will not be published. Required fields are marked *




