

Menorrhagia (Heavy Menstrual Bleeding): Causes, Diagnosis, and Treatment
Introduction
Menorrhagia, or heavy menstrual bleeding, refers to periods lasting more than 7 days or involving blood loss greater than 80 ml per cycle. While it can occur at any age, it is most common in women between 30 and 40 years old. Frequent and prolonged bleeding can lead to anemia, chronic fatigue, low energy, and disruption of daily activities. Many women also struggle with anxiety, loss of confidence, and social limitations due to worries about staining or lack of control over bleeding. Understanding the causes, diagnostic steps, and treatment options can significantly improve quality of life.
Definition and Types of Menorrhagia
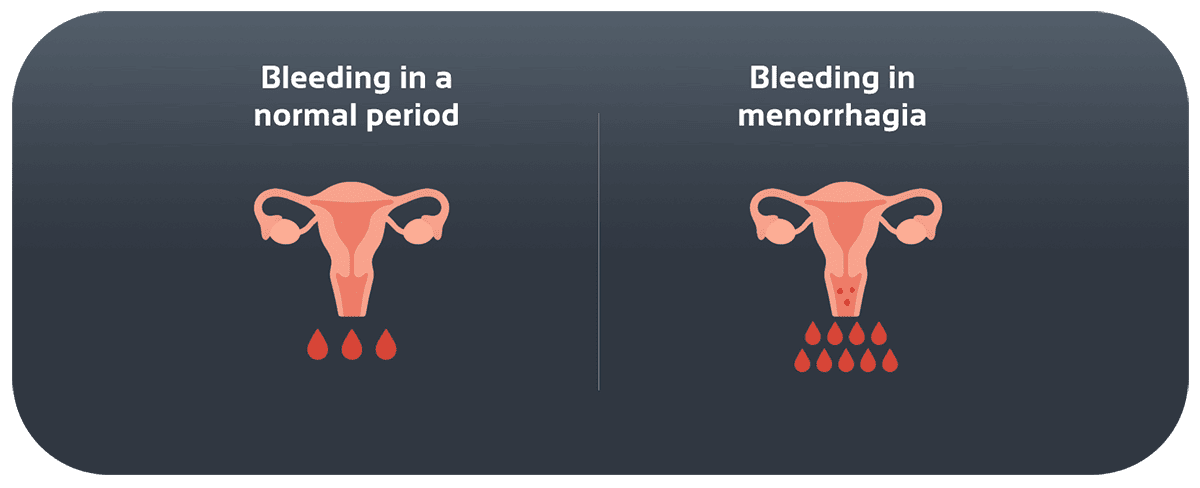
True menorrhagia is defined as bleeding greater than 80 ml per cycle or lasting more than 7 days. In contrast, “perceived menorrhagia” refers to when a woman feels her bleeding is heavy, but careful measurement of blood loss or pad count shows it is within normal range. Differentiating between the two is key for proper management.
Symptoms and Consequences

Heavy menstrual bleeding may be a sign of underlying disorders and carries important health consequences. Common symptoms include:
- Changing pads or tampons every 1–2 hours
- Dizziness, weakness, or fatigue
- Spotting between cycles
- Severe abdominal cramps
Prolonged blood loss often leads to iron deficiency anemia, causing exhaustion, poor concentration, and heart palpitations. The condition also impacts work, social life, and emotional wellbeing, sometimes leading to embarrassment and anxiety.
Causes of Menorrhagia
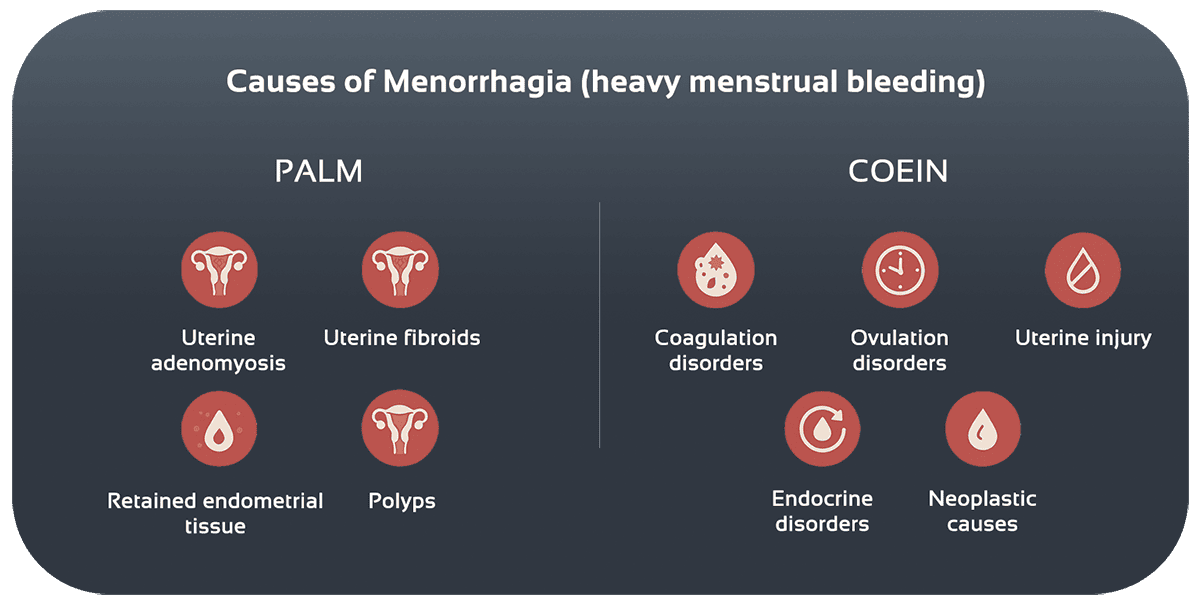
The causes of menorrhagia are often summarized by the acronym **PALM**:
- Polyp: Benign growths in the uterus lining causing irregular bleeding
- Adenomyosis: Endometrial tissue growing into the uterine muscle, leading to heavy, painful periods
- Leiomyoma (Fibroids): Benign uterine tumors that increase bleeding depending on size and location
- Malignancy or retained tissue: Residual endometrial tissue after miscarriage or delivery can also cause prolonged bleeding
If the uterus appears structurally normal, causes fall under **COEIN**:
- **Coagulopathy:** Clotting disorders such as von Willebrand disease
- **Ovulatory dysfunction:** Hormonal imbalance leading to excess thickening of the uterine lining
- **Endocrine disorders:** Thyroid dysfunction and other hormonal imbalances
- **Iatrogenic (Trauma or Medication):** Uterine injury, prolapse, or use of anticoagulant drugs
- **Neoplastic causes** (less common but important to consider)
Diagnosis
Accurate diagnosis combines medical history, physical examination, and additional tests:
- Careful review of bleeding patterns, medication use, family history, and associated symptoms
- Pelvic exam and transvaginal ultrasound to detect fibroids, polyps, or endometrial thickness
- Blood tests including CBC (for anemia), thyroid function (TSH), and clotting studies
- Endometrial biopsy for women at risk of cancer or with persistent symptoms
Treatment and Management
Medication Options
- Combined oral contraceptives: regulate hormones and reduce bleeding
- Levonorgestrel-releasing IUS (intrauterine system): reduces bleeding by up to 80%
- NSAIDs: lower prostaglandin levels and ease pain
- For bleeding disorders: agents like desmopressin may be prescribed
Non-Drug Approaches
- Iron-rich diet with vitamin C for better absorption
- Heat therapy with hot packs or warm baths
- Gentle exercise, yoga, and walking to improve pelvic circulation
- Natural stress management techniques to reduce inflammation
Surgical Options
If conservative treatments fail or pregnancy is not desired:
- **Endometrial ablation:** destroys uterine lining to reduce bleeding
- **Myomectomy:** removes fibroids while preserving the uterus
- **Hysterectomy:** removal of the uterus, considered the last option for severe, resistant cases
Related Conditions
Menorrhagia is often linked to adenomyosis, endometriosis, and uterine fibroids. Coagulation disorders such as von Willebrand disease should also be considered, especially in women with no structural uterine causes.
Case Examples
- A 30-year-old woman with a large posterior uterine fibroid reported blood loss of over 120 ml per cycle. After laparoscopic myomectomy, her bleeding reduced to about 30 ml, and hemoglobin improved from 9.5 to 12 g/dL.
- A 28-year-old woman with vitamin K deficiency experienced severe menorrhagia. After treatment with vitamin K and iron supplements plus a levonorgestrel IUS, she reported a 65% reduction in bleeding within three cycles.
Prevention and Self-Care Tips
- Eat a balanced diet with iron-rich foods (meat, spinach, legumes) and vitamin C
- Start NSAIDs 1–2 days before menstruation to reduce bleeding and cramps
- Maintain regular physical activity like walking or light exercise
- Get annual pelvic ultrasounds and blood tests, especially if there’s a family history of uterine problems
Conclusion
Menorrhagia, or heavy menstrual bleeding, has wide-ranging physical and psychological effects. Identifying the underlying cause, choosing the right treatment, and regular follow-up are key to improving quality of life. If you experience prolonged or heavy bleeding, consult a gynecologist promptly.
References

Heavy bleeding isn’t normal; find your treatment plan.
Fill out the consultation form now and our assistant will contact you shortly.
 FAQ
FAQ
No comments have been posted.
Your email address will not be published. Required fields are marked *




