

Perineorrhaphy; Perineal Repair and Rejuvenation of the Vaginal Entrance
Introduction
After vaginal childbirth or simply over time, many women notice changes in the perineum—the area between the vaginal opening and the anus. The perineum may tear, become lax, or look irregular. These changes can alter the appearance of the genital area and may affect sexual function, the sense of vaginal control, and self-confidence.
Perineorrhaphy is a restorative, aesthetic procedure that tightens the vaginal entrance and rejuvenates the perineum by reinforcing and suturing the perineal muscles and refining the introitus.
What is the perineum and why does it matter
The perineum is the skin-and-muscle region between the vaginal opening and the anus. It can be damaged or lose elasticity after vaginal delivery, with menopause, or simply due to aging.
Key roles of the perineum:
- Supports the vaginal entrance and pelvic organs
- Contributes to muscular control of the vagina
- Directly influences intimate appearance and sexual function
When the perineum becomes lax or injured, many patients feel the vagina is “open” or “loose,” and the entrance may look irregular.
What is perineorrhaphy
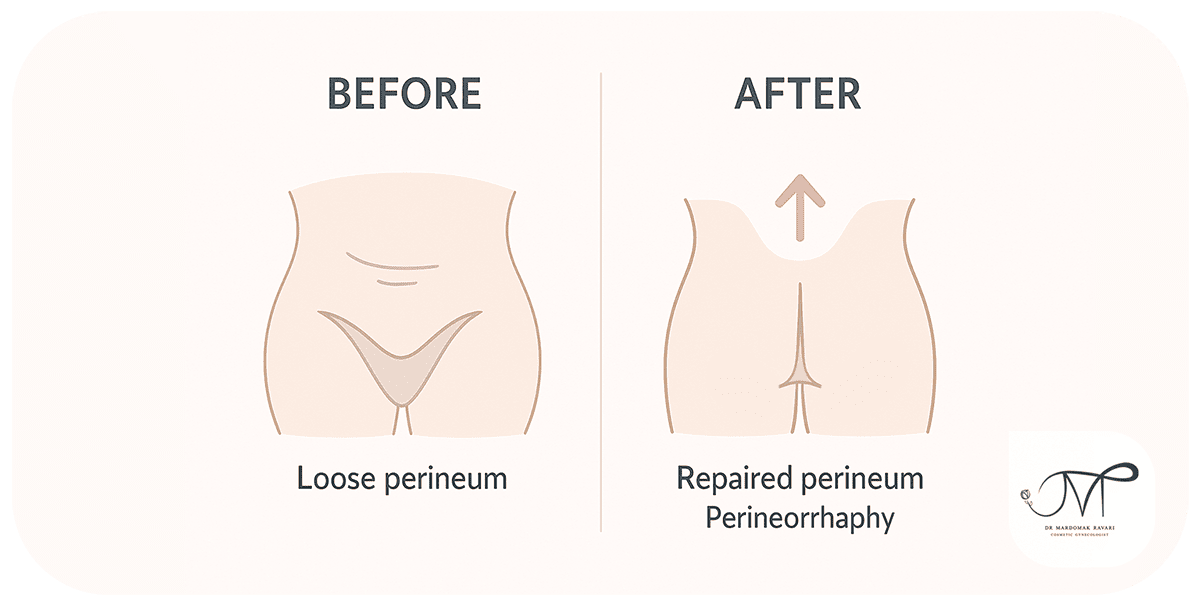
Perineorrhaphy is a restorative and cosmetic procedure focused on the perineum (the area between the vagina and anus). Its main goal is to correct perineal laxity and tears while strengthening the vaginal entrance.
In very simple terms:
Perineorrhaphy means bringing the loosened perineal muscles and tissues back together and suturing them so the vaginal opening feels firmer, the entrance looks neater, and problems from poorly healed childbirth tears are corrected.
Where exactly is the perineum and why is it important
- It is the muscular-skin bridge between the vaginal opening and the anus.
- During vaginal birth it is stretched or torn. If it is not repaired well, it can:
- Leave the vaginal entrance looser and more open,
- Create an irregular appearance or noticeable scar,
- And affect sexual comfort and relationship quality.
Perineorrhaphy helps restore both the appearance and the functional support of this region.
How perineorrhaphy differs from vaginoplasty
- Vaginoplasty focuses on the inside of the vaginal canal and is used more for moderate to severe vaginal laxity.
- Perineorrhaphy targets the entrance and the perineum.
- In many patients, both are done together to refine the canal and the opening for a more complete result.
Problems perineorrhaphy can address
- A loosened vaginal entrance after childbirth
- Poorly healed episiotomy or obstetric tears
- Irregular appearance or problematic perineal scars
- A sense of openness or reduced friction during intercourse
- Pain during sex caused by scar tissue or perineal descent
Goals of perineorrhaphy
- A snugger vaginal entrance and a restored sense of firmness
- Reinforcement of the perineal muscles and improved pelvic floor support
- Smoother, neater perineal appearance with revision of old scars
- Greater sexual satisfaction and confidence for many patients
Who is a good candidate
Perineorrhaphy is not necessary for everyone. In specific situations, it can be the best option to restore the natural look, strengthen the introitus, and improve sexual comfort.
1) Women with vaginal delivery
- The perineum bears the most stretch in childbirth.
- It may tear or be cut (episiotomy), and if the initial repair was not ideal, laxity and irregular scars can remain.
- This group is the most common candidate.
2) Those unhappy with a persistent “open” feeling
- Some women, even without childbirth, gradually feel the opening is not snug due to genetics or time.
- This can reduce friction in intercourse.
- Perineorrhaphy tightens the perineal ring and restores support.
3) People with problematic scars or incomplete healing
- Some episiotomy or tear scars heal raised, depressed, or crooked, causing pulling with sitting, walking, or intimacy.
- Perineorrhaphy can refine scars and improve both look and comfort.
4) Women reporting reduced sexual pleasure
- Laxity of the perineum and introitus can reduce friction during sex.
- Many couples report better satisfaction after perineorrhaphy.
5) Women in menopause or later life
- Lower estrogen thins tissues and reduces tone, even without prior births.
- Perineorrhaphy can restore firmness; dryness should be treated separately with hormonal or lubricant options.
6) Patients seeking aesthetic improvement
- Some primarily want a tidier, more youthful-looking entrance.
- Combined with labiaplasty or vaginoplasty, the overall appearance can look more harmonious.
7) Women with day-to-day functional concerns
- Laxity can reduce the sense of control at the opening.
- Some experience discomfort with tampons or during exercise.
- These patients may benefit as well.
Who is not currently a candidate
- Active vaginal or skin infection (treat first)
- Plans for pregnancy soon (a future birth can change the result)
- Uncontrolled medical issues (such as advanced diabetes or bleeding disorders)
- Unrealistic expectations (for example, expecting surgery to solve all sexual issues by itself)
A good candidate typically
- Has perineal laxity or tearing after vaginal birth,
- Dislikes a sense of openness or reduced friction,
- Has problematic scarring or irregular healing,
- Is unhappy with the look of the perineum and entrance,
- Or seeks coordinated improvement alongside other cosmetic gynecologic procedures.
Common reasons why perineorrhaphy is recommended
Perineorrhaphy is suggested when the perineum has become lax, damaged, or irregular—affecting appearance, function, and sexual comfort. Below are key causes in plain language, along with common signs patients notice.
1) Obstetric tear or episiotomy with suboptimal repair
Cause
During vaginal birth, the perineum stretches; sometimes an episiotomy is made to avoid irregular tearing. If the tear was deep or the initial suturing was not precise, long-term laxity or asymmetry can persist.
Typical signs
– A feeling that the entrance is “too open” or not snug
– Less friction and reduced sexual satisfaction
– A misshapen scar, pulling, or pinpoint pain during intimacy
– Occasional vaginal flatulence (air trapping with exercise or sex)
Why perineorrhaphy helps
By re-approximating the perineal muscles and smoothing the skin and scar, the entrance becomes tighter and more natural. Scar-related pain often improves if the cause truly is the scar.
2) Laxity after multiple births or large babies
Cause
Repeated or prolonged labor and higher-birth-weight infants can weaken perineal fibers even without a major tear.
Typical signs
– Reduced control at the entrance
– Needing more effort to keep a tampon in place
– Less friction for the patient or partner
Why perineorrhaphy helps
Reinforcing the muscular ring at the introitus restores support and a snugger feel.
3) Painful or irregular childbirth scars
Cause
Some scars heal raised, indented, or off-axis and pull during movement or sex.
Typical signs
– Pinpoint pain with sex, touch, or even tight clothing
– Irregular, bothersome appearance
Why perineorrhaphy helps
Scar revision and tissue rebalancing relieve pressure on sensitive nerves and improve symmetry.
4) Aging and menopause
Cause
Lower estrogen reduces collagen and firmness; the perineum can thin and loosen even without birth history.
Typical signs
– A looser entrance
– Subtle wrinkling or descent of the perineum
– Possible vaginal dryness (treat separately with hormones or gels)
Why perineorrhaphy helps
It restores mechanical support; combine with topical estrogen or energy-based therapies to address dryness.
5) Chronic straining, cough, or high-impact activity
Cause
Repeated intra-abdominal pressure gradually stretches the pelvic floor and perineum.
Typical signs
– A sense of weakness and laxity
– Mild posterior vaginal wall bulge in some
– Difficulty retaining tampons or a feeling of openness
Why perineorrhaphy helps
Surgical reinforcement re-supports the entrance; managing the underlying strain (constipation, cough, technique) preserves results.
6) Genetic tissue quality
Cause
Some individuals naturally have softer connective tissue and lower collagen strength.
Typical signs
– Earlier-than-expected perineal laxity
– Mild opening and reduced friction
Why perineorrhaphy helps
Strengthening the entrance improves control; post-op Kegels help maintain the outcome.
7) Aesthetic concerns
Cause
Some dislike a sagging, asymmetric, or hollowed perineal look even without pain.
Typical signs
– Dissatisfaction with appearance and lower confidence
– Avoiding fitted swimwear or clothing
Why perineorrhaphy helps
By refining skin and reinforcing the entrance, the area looks tidier and more youthful; often combined with labiaplasty or vaginoplasty.
8) Intercourse-related issues: pain, pulling, or reduced satisfaction
Cause
Laxity can reduce friction, while a misaligned scar can cause focal pain.
Typical signs
– Lower pleasure due to mechanical laxity
– Point tenderness at the scar or skin stretch
Why perineorrhaphy helps
By tightening the ring and revising scars, the mechanical problem is addressed; psychological or hormonal factors should be treated alongside if present.
9) Mild posterior wall support issues
Cause
In early or mild posterior wall laxity, perineorrhaphy can improve introitus support; moderate to severe prolapse requires pelvic floor surgery.
Typical signs
– A mild posterior bulge
– A clearly loose introitus
Why perineorrhaphy helps
Useful in mild cases; higher grades need specialized evaluation.
Signs you may benefit
- A persistent sense of openness and lack of snugness
- Mechanically reduced friction and satisfaction during sex
- A painful or irregular entrance scar
- Difficulty retaining tampons or air entry during exercise
- Dissatisfaction with the perineal look (sagging or asymmetry)
A careful exam determines whether perineorrhaphy alone is sufficient or if it should be combined with vaginoplasty or labiaplasty.
Important boundaries: what perineorrhaphy alone does not treat
- Moderate to severe pelvic organ prolapse of the uterus, bladder, or rectum
- Menopausal vaginal dryness (treat with hormones or lubricants)
- Disorders of desire or orgasm (primarily hormonal or psychological; surgery is not a direct fix)
Brief examples
Mina, 33: two births; first-birth stitches healed poorly. Signs: pinpoint pain at the entrance plus irregular look. Solution: perineorrhaphy to revise the scar and reinforce the opening.
Nahid, 39: multiple births and a sense of laxity with less friction. Solution: perineorrhaphy alone or with vaginoplasty based on the exam.
Elham, 47: menopausal, mild laxity with aesthetic concern. Solution: perineorrhaphy plus hormone-based care or topical gel for dryness.
Summary of indications
Most common reasons include:
- Tear/episiotomy with imperfect repair,
- Laxity after multiple births or large babies,
- Painful or irregular scars,
- Menopausal or age-related changes,
- Chronic pressure from straining or coughing,
- Genetic tissue softness and aesthetic or functional dissatisfaction.
Perineorrhaphy tightens the muscular ring and refines the skin for a neater, more supported entrance. Broader pelvic floor problems or hormone-related dryness may need additional therapies.
How perineorrhaphy is performed (surgical steps)
- Examination and marking: assess perineum, old scars, and degree of laxity
- Local anesthesia or short general anesthesia as needed
- Small perineal incision to access the muscles
- Plication of the muscles: bringing loosened perineal muscles together and reinforcing them
- Scar revision or trimming of redundant tissue when needed
- Fine absorbable sutures to close the skin and reshape the entrance
Typical duration is about 30 to 60 minutes and it is often an outpatient procedure.
Benefits
- A tighter entrance with a more supported feel
- Improved friction and sexual comfort for many couples
- Correction of irregular or painful scars
- A more youthful, harmonious appearance at the introitus
- Greater relationship confidence
- Relief of pain when the cause is scarring or mechanical laxity
Possible downsides and risks
- Several days of soreness, swelling, and bruising
- Bleeding or infection (uncommon with proper care)
- Internal scarring (generally concealed and improves with time)
- Over-tightening can cause painful intercourse if done excessively
- Temporary abstinence from sex and heavy activity (about six weeks)
Pre- and post-procedure care
- Before surgery
- Treat any vaginal infections first
- Stop smoking 2 to 4 weeks before
- Pause blood thinners as advised by your doctor
- Trim hair with a clipper rather than close shaving
After surgery
- Relative rest for the first 2 to 3 days
- Gentle cold compresses for the first 48 hours
- Rinse with lukewarm water and pat dry
- Wear loose cotton underwear
- Avoid prolonged sitting, swimming, and sex for about six weeks
- Seek care promptly for fever, foul discharge, or unusual bleeding
Patient experiences
Maryam, 34: “After my first birth I always felt the opening hadn’t closed. My confidence was low during intimacy. After perineorrhaphy, the entrance looks neat and sex feels much better.”
Elham, 40: “My second-birth episiotomy healed badly and always hurt. Perineorrhaphy revised the scar and the pain is gone.”
Niloufar, 28: “I was newly married and unhappy with the look of my perineum. The procedure was quick, and by two months the area looked much better and my confidence grew.”
Conclusion
Perineorrhaphy is an effective option for correcting perineal laxity and birth-related injuries. It can tighten the entrance, revise poorly healed scars, and, for many, improve sexual comfort and confidence. Choosing an experienced surgeon and following aftercare instructions are the keys to success.
Similar Articles

Regain confidence and comfort in intimacy!
Fill out the consultation form now and our assistant will contact you shortly.
 FAQ
FAQ
No comments have been posted.
Your email address will not be published. Required fields are marked *




