
Bladder Prolapse Repair; Treating Cystocele and Urinary Incontinence
Introduction
Bladder prolapse, also called cystocele, is common in women, especially after multiple vaginal births or with aging. In this condition, the muscles and tissues that support the bladder weaken, and the bladder shifts downward toward the vagina. Beyond physical discomfort such as urinary leakage or a heavy pelvic feeling, cystocele can reduce quality of life and confidence. The good news: today there are effective ways to repair bladder prolapse, from simple non-surgical therapies to advanced surgeries.
What is bladder prolapse
Normally, the bladder is held in place by a strong network of pelvic floor muscles and ligaments, much like a supportive spring mattress that keeps pelvic organs where they belong. When these supports are stretched, weakened, or injured, the bladder descends toward and into the vagina. This is called bladder prolapse or cystocele.
In simple terms: bladder prolapse means the bladder sits lower than it should and presses into the vaginal canal.
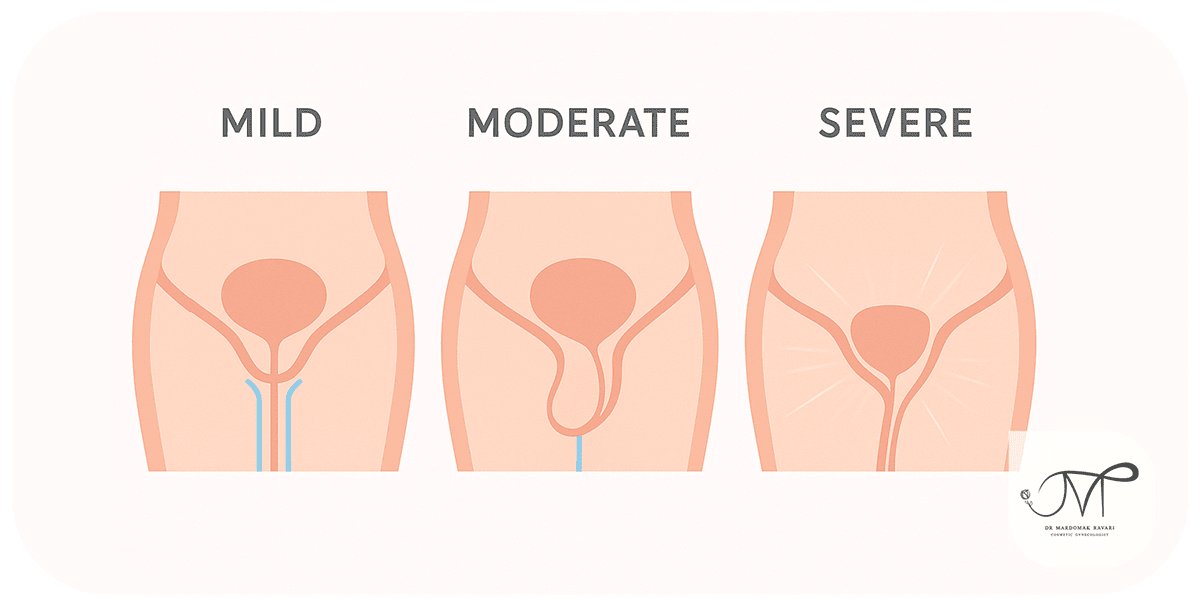
Degrees of bladder prolapse
- Mild: the bladder sags slightly toward the vagina. Symptoms are often subtle, such as urinary frequency or a mild pressure sensation.
- Moderate: part of the bladder bulges into the vagina. Symptoms are more bothersome, such as stress incontinence or pelvic pain.
- Severe: the bladder visibly protrudes out of the vaginal opening. Surgery is usually required at this stage.
Why does it happen
– Difficult or multiple vaginal deliveries that strain or injure the pelvic floor
– Menopause and lower estrogen, which thins and weakens tissues
– Aging, which reduces muscle tone and ligament strength
– Obesity or chronic constipation that increases pressure on the pelvic floor
– Chronic cough in smokers or lung disease, which repeatedly raises abdominal pressure
Symptoms of bladder prolapse
– A feeling of pelvic pressure or heaviness
– A bulge inside the vagina that may be felt or seen
– Urine leakage with coughing, sneezing, or exercise
– Urinary frequency or a sensation of incomplete bladder emptying
– Discomfort or pain during sexual activity
– Low back ache or a pulling sensation in the pelvis
Note: symptom severity often tracks with prolapse grade.
How it is diagnosed
– Pelvic exam by a gynecologist to assess support and bulge
– Pelvic ultrasound to evaluate prolapse and other organs when needed
– Urodynamic testing in selected cases to study bladder function
– MRI in complex or unclear cases for detailed pelvic floor imaging
Bladder Prolapse Treatment and repair options

- Non-surgical care for mild cases
– Kegel exercises: targeted pelvic floor strengthening
– Specialized pelvic floor physical therapy: may include biofeedback or neuromuscular stimulation
– Vaginal pessary: a medical silicone device placed in the vagina to support the bladder
– Local vaginal estrogen: especially helpful after menopause to improve tissue quality
- Surgical care for moderate to severe cases
Anterior colporrhaphy
– The most common operation for cystocele
– Performed through the vagina by opening the anterior vaginal wall, tightening and plicating the weakened tissues, and restoring bladder position
– Highly effective for mild to moderate prolapse
Mesh-augmented repair
– Considered when native tissues are very weak or the risk of recurrence is high
– A medical mesh reinforces the anterior vaginal wall like a scaffold
– Must be performed by an experienced surgeon and with modern, regulated mesh systems to minimize complications
Combined repairs
– Prolapse of the bladder may coexist with uterine or rectal prolapse
– Surgeons may correct multiple defects in one session, for example cystocele repair plus hysterectomy or rectocele repair, to address all issues comprehensively
Surgery step by step
- Anesthesia, either general or spinal, based on individual factors
- A small incision in the front vaginal wall
- Repositioning the bladder to its anatomical location
- Tightening and reinforcing the fascia and tissues, with or without mesh
- Closing the incision
Typical operating time is 1 to 2 hours. Most patients stay one night and go home the next day.
After surgery

– Relative rest for the first weeks
– Avoid sexual intercourse and heavy lifting for 4 to 6 weeks
– Take prescribed antibiotics and anti-inflammatory medications as directed
– Resume pelvic floor exercises after healing to prolong results
Pros and cons of surgery
Pros
– Durable, definitive correction
– Relief of incontinence and pelvic pressure
– Better quality of life and more comfortable intimacy
Cons
– Requires anesthesia and a short hospitalization
– Several weeks of recovery
– Possibility of recurrence over time, especially without lifestyle changes
– Small risks such as infection, bleeding, or temporary discomfort
Patient stories
Fatemeh, 52
I struggled for years with leakage and pelvic pressure. I tried Kegels and a pessary but they did not solve it. I finally had anterior colporrhaphy. Six months later, I am symptom-free. I can walk, exercise, and my intimate life is back to normal. The only challenge was being careful during recovery.
Nasrin, 45, after three vaginal births
After my third delivery, I felt a bulge and pressure in my vagina, even when walking. Exam showed bladder prolapse. Surgery took about an hour and I went home the next day. Two months later my body felt like itself again. No more incontinence and no more heavy pressure.
Maasoumeh, 57, menopause with severe leakage
After menopause I developed frequent urination and loss of control when sneezing. Exam confirmed severe prolapse. I had anterior colporrhaphy. Recovery took some patience, but a year later I have no problems and feel confident in social situations.
Elham, 38, severe cystocele with uterine descent
I had both bladder and mild uterine prolapse. My surgeon recommended a combined repair. I was nervous, but the outcome exceeded expectations. Six months later, life is normal and sex is comfortable and pain-free.
Bottom line
Surgical bladder repair is the best choice for severe or recurrent prolapse. While recovery takes a few weeks, the result is usually long-lasting and very satisfying.
Pros and cons of non-surgical versus surgical care
Non-surgical
– Pros: safe, no anesthesia, suitable for mild prolapse
– Cons: limited effect in moderate to severe cases
Surgical
– Pros: more definitive and durable
– Cons: anesthesia, recovery period, potential for recurrence over years
Self care and prevention
– Do Kegel exercises consistently
– Maintain a healthy weight
– Treat constipation and avoid straining
– Avoid lifting heavy loads
– Stop smoking to reduce chronic cough
– Schedule follow ups with your doctor after childbirth or surgery
More patient experiences
Zahra, 48
After three vaginal deliveries I had stress incontinence. Surgical bladder repair fixed it and I can exercise without worry.
Leila, 36
My prolapse was mild. With Kegels and pelvic physio I improved a lot and do not need surgery for now.
Mahtab, 55
After menopause I felt pressure in the vagina. A pessary controlled my symptoms and I chose to postpone surgery.

Bladder prolapse isn’t scary if treated early.
Fill out the consultation form now and our assistant will contact you shortly.
 FAQ
FAQ
No comments have been posted.
Your email address will not be published. Required fields are marked *




