
Dysmenorrhea (Painful Periods): Causes, Diagnosis, and Treatment Options
Introduction
Dysmenorrhea, or painful periods, is a common problem among women of reproductive age. It usually presents as cramping and pain in the lower abdomen or pelvis during menstruation. The pain often starts on the first day of bleeding and can range from mild discomfort to severe, disabling pain.
In addition to cramps, some women may experience nausea, dizziness, or fatigue. Severe menstrual pain can negatively affect quality of life, daily activities, and even mental health. That’s why understanding the causes, underlying mechanisms, and effective treatment options is essential for women’s health and wellbeing.
Types of Dysmenorrhea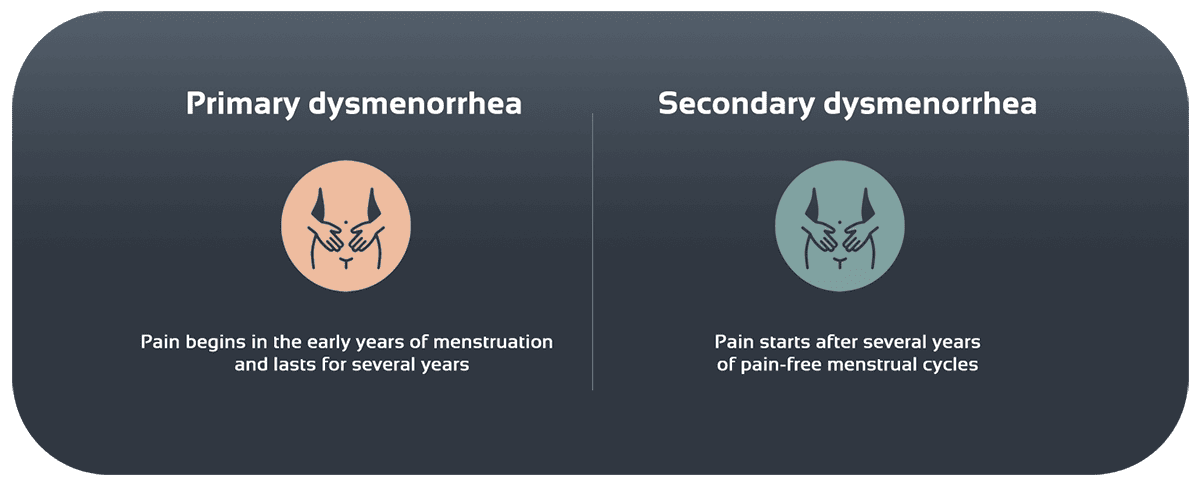
-
Primary Dysmenorrhea
- Pain starts early in menstrual life (soon after menarche) and continues for years.
- Cause: Excess prostaglandins in the uterine lining that trigger strong contractions and temporary reduced blood flow.
- Features: Pain begins with or just before bleeding, recurs monthly, and usually responds well to NSAIDs.
-
Secondary Dysmenorrhea
- Pain develops after years of painless periods.
- Cause: Underlying conditions such as endometriosis, fibroids, adenomyosis, or pelvic inflammatory disease (PID).
- Features: Pain lasts longer (more than 3–4 days), is resistant to common treatments, and often comes with chronic symptoms between periods.
Symptoms and Characteristics
Besides pelvic pain, dysmenorrhea can cause:
- Nausea and vomiting – due to nervous system stimulation
- Diarrhea or constipation – from the uterus–gut connection
- Dizziness and weakness – linked to low blood pressure and inflammation
- Fatigue – sometimes due to mild or moderate anemia
- Back and thigh pain – pain spreading from the uterus to surrounding tissues
The more severe the secondary dysmenorrhea, the stronger and longer-lasting these symptoms may be.
Causes of Dysmenorrhea
Primary Dysmenorrhea
- Prostaglandins: High levels of PGF₂α and PGE₂ cause repeated and strong uterine contractions.
- Inflammatory response: Cytokine release in the uterine lining increases nerve sensitivity.
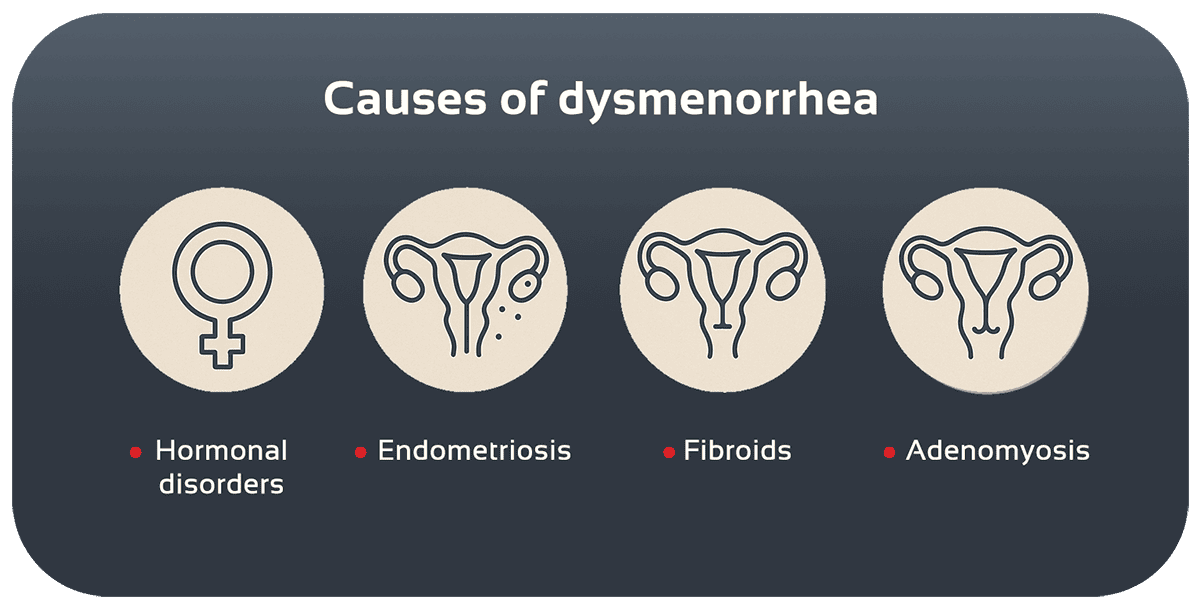
Secondary Dysmenorrhea
- Endometriosis: Growth of endometrial-like tissue outside the uterus, causing inflammation and adhesions.
- Uterine Fibroids: Benign muscle tumors that increase bleeding and pelvic pressure.
- Adenomyosis: Endometrial tissue grows into the muscle wall of the uterus, causing heavy bleeding and pain.
- Pelvic Inflammatory Disease (PID): Chronic infections that lead to adhesions and pelvic pain.
Diagnosis Methods
- Detailed history: Timing, duration, severity, and relieving or worsening factors.
- Physical and pelvic exam: Checking for tenderness, masses, or uterine abnormalities.
- Transvaginal ultrasound: Detecting cysts, fibroids, or adenomyosis.
- Pelvic MRI: For unclear ultrasound findings.
- Laparoscopy: Gold standard for diagnosing endometriosis and removing lesions.
- Blood tests: CBC for anemia, CRP and ESR for inflammation.
Treatment and Management
Medication Options
- Mefenamic acid and magnesium, starting 3 days before periods.
- NSAIDs (ibuprofen, naproxen): Block COX enzyme and reduce prostaglandins.
- Combined oral contraceptives: Balance hormones and thin the uterine lining.
- Intrauterine system (LNG-IUS): Releases progesterone locally, reducing bleeding by up to 80%.
Non-Drug Options
- Heat therapy: Hot water bottle or warm bath.
- Physiotherapy and massage: Relieves pelvic muscle tension.
- Gentle exercise and yoga: Improve blood flow and reduce spasms.
- Natural anti-inflammatories: Omega-3s, ginger, turmeric.
Surgical Options
- Laparoscopic surgery: Removal of endometriosis or small fibroids.
- Endometrial ablation: Destroying uterine lining to reduce bleeding.
- Hysterectomy: Removing the uterus in severe, resistant cases.
Related Conditions
- Endometriosis – endometrial tissue outside the uterus
- Uterine Fibroids – benign growths
- Adenomyosis – endometrial tissue inside uterine muscle
- Irritable Bowel Syndrome (IBS) – overlapping digestive and pelvic pain
Clinical Case Examples
- 21-year-old with primary dysmenorrhea: After regular NSAID use, reported 50% reduction in pain over three cycles.
- 36-year-old with endometriosis: After laparoscopy and hormone therapy, pain scores improved from 7/10 to 2/10.
Prevention Tips

- Start NSAIDs one day before menstruation to prevent cramps.
- Follow an anti-inflammatory diet: fruits, vegetables, whole grains.
- Stay active with walking, swimming, or yoga.
- Manage stress with meditation and breathing exercises.
Conclusion
Dysmenorrhea may be common, but when it interferes with daily life, it requires medical evaluation and treatment. A combination of medication, non-drug approaches, and sometimes surgery can restore quality of life. If you struggle with painful periods, consult a gynecologist for proper care.
References

Don’t let period pain disrupt your life;
Fill out the consultation form now and our assistant will contact you shortly.
 FAQ
FAQ
No comments have been posted.
Your email address will not be published. Required fields are marked *




