

Uterine Adhesions (Asherman’s Syndrome) | Symptoms, Causes and Treatments
Introduction: What are uterine adhesions
Uterine adhesions, or Asherman’s syndrome, occur when the inner walls of the uterus stick together, reducing or blocking the uterine cavity. This condition often develops after uterine surgery or severe infection. Adhesions may lead to decreased or absent menstruation, infertility, or recurrent miscarriage. Early detection is crucial, as timely treatment significantly increases the chances of successful pregnancy.
Causes and risk factors
The main causes include:
- Dilation and curettage (D&C) after miscarriage or childbirth: the most common cause, especially with deep curettage.
- Uterine surgeries: such as removal of fibroids or polyps.
- Severe uterine infections: for example, genital tuberculosis or postpartum infections.
- Cesarean section or pelvic surgery: which may sometimes damage the uterine wall.
- Rare causes: pelvic radiotherapy or medical device-related injury.
Symptoms and signs
Depending on severity and location, symptoms vary:
- Reduced menstrual flow or complete absence of periods.
- Cyclic pelvic pain without bleeding (due to trapped blood).
- Infertility or recurrent miscarriages.
- Occasionally recurrent uterine infections.
Note: Some women have no obvious symptoms, and adhesions are only discovered during infertility evaluation.
Diagnosis
Doctors often combine imaging and direct visualization:
- Transvaginal ultrasound: evaluates uterine shape and lining.
- Hysterosalpingography (HSG): an X-ray using contrast dye to show blockages or adhesions.
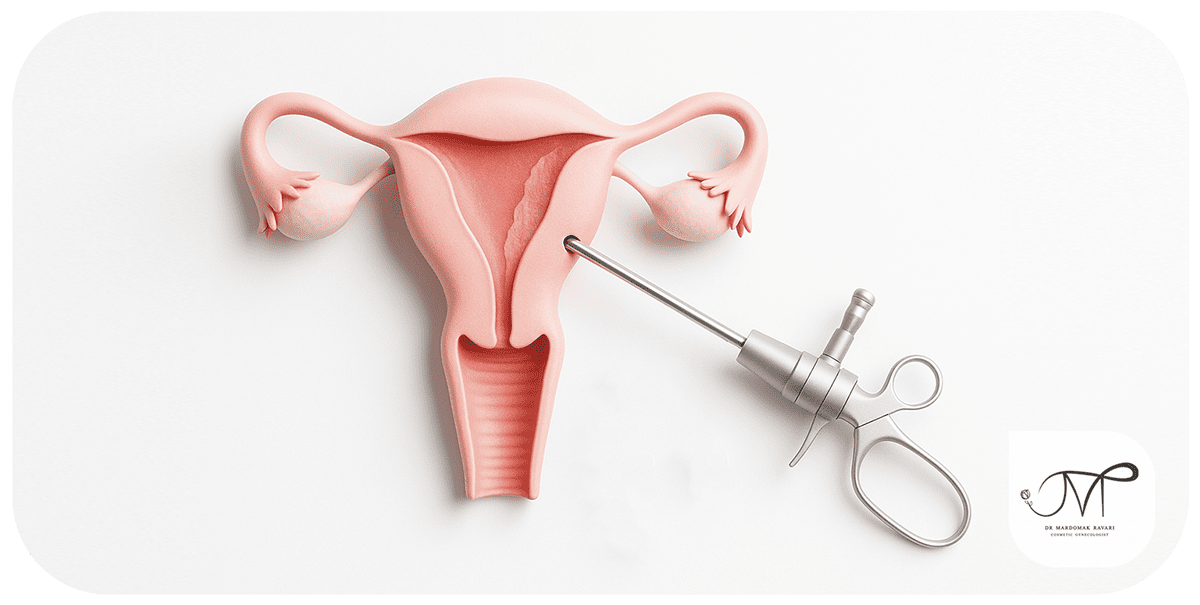
- Hysteroscopy: the gold standard; a small camera inserted into the uterus allows direct visualization of adhesions.
Complications
- Infertility or difficulty conceiving.
- Recurrent pregnancy loss.
- Increased risk of abnormal placentation (such as placenta previa) in future pregnancies.
- Chronic pelvic pain.
Treatment
-
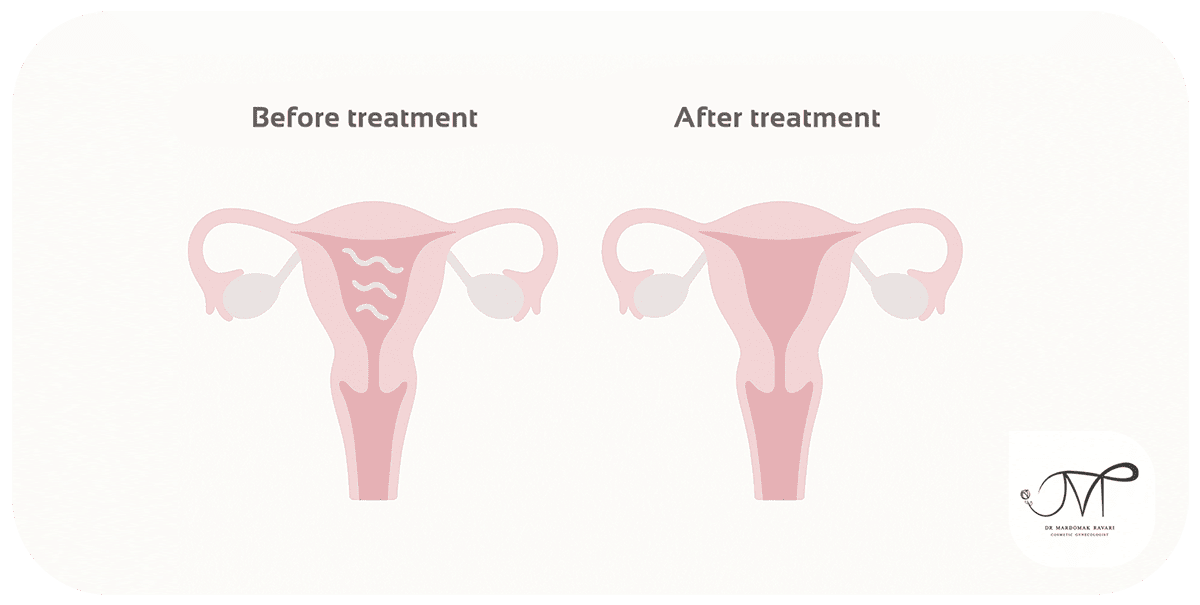
Surgical hysteroscopy
- The most effective treatment.
- Fine instruments are used to cut adhesions and restore the cavity.
- A balloon or special IUD may be placed temporarily to prevent re-adhesion.
-
Medications
- Estrogen therapy helps regenerate the uterine lining after surgery.
- Antibiotics are used when infection is present.
-
Post-treatment care
- Regular follow-up after surgery.
- Monitoring with ultrasound or repeat hysteroscopy when needed.
Prevention and self-care

Uterine adhesions cannot always be prevented, but risks can be reduced:
- Perform D&C only when necessary, by skilled specialists
- D&C is a major cause. Avoiding unnecessary procedures reduces risk.
- Alternatives such as medication-based uterine evacuation may be preferable in some cases.
- Prompt treatment of uterine infections
- Severe infections can trigger adhesions.
- Symptoms like foul discharge, fever, pelvic pain, or abnormal bleeding require immediate medical attention.
- Follow-up after uterine surgery
- Any uterine operation, including fibroid removal, polyp removal, or cesarean section, carries risk.
- Monitoring for amenorrhea or unusual pain is essential.
- Preventive use of IUDs, balloons, or hormones may reduce recurrence.
- Seek medical advice for sudden menstrual changes
- Abruptly lighter or absent periods may be an early sign of adhesions.
- Early diagnosis allows simpler, more effective treatment.
Pregnancy with IVF in Patients with Uterine Adhesions
For women with severe uterine adhesions (Asherman’s syndrome) where surgical treatments have failed to fully restore the uterine cavity, one effective option for pregnancy is in vitro fertilization (IVF). This method allows physicians to bypass the natural implantation pathway in a damaged uterus, increasing the chances of conception.
Purpose f IVF in Patients with Uterine Adhesions
The main goal is to enhance the likelihood of creating a healthy embryo and transferring it to a restored uterus or a surrogate (in specific cases). In many patients, ovarian function remains normal and ovulation occurs regularly. Therefore, the primary problem lies in the uterine environment for implantation, not in egg or sperm quality.
Steps of IVF in These Patients
1. Uterine Evaluation and Preparation
– Before IVF, the doctor assesses the uterine cavity using ultrasound and hysteroscopy.
– If adhesions are repairable, surgical hysteroscopy is performed to create sufficient space for embryo implantation.
– Hormonal therapy with estrogen and progesterone is usually prescribed for several weeks to thicken the endometrial lining and improve receptivity.
– If the uterus remains unsuitable for embryo transfer after several treatments, the doctor may suggest a surrogate uterus.
2. Ovarian Stimulation and Egg Retrieval
– Fertility medications are used to stimulate multiple follicles.
– When follicles reach the appropriate size, eggs are retrieved from the ovaries using a puncture procedure.
3. Laboratory Fertilization and Embryo Culture
– Eggs are fertilized with the partner’s sperm in the lab, and embryos are cultured until day 3 or 5.
– Healthy, high-quality embryos are selected for transfer.
4. Embryo Transfer
– If the patient’s uterus is ready, embryos are transferred directly.
– If the uterine environment is not optimal, embryos are frozen for future transfer after full uterine restoration.
– In some cases, embryos are transferred to a surrogate’s uterus.
IVF Success in Patients with Uterine Adhesions
Success depends on several factors:
– Severity and extent of adhesions: Better restored uterine cavities improve success rates.
– Endometrial thickness after treatment: An endometrium above 7 mm is ideal for implantation.
– Patient age and egg quality: Crucial determinants for IVF outcomes.
– Absence of infection or active inflammation: A healthy uterine environment is essential before transfer.
Generally, mild to moderate adhesions can result in 40–50% pregnancy rates with IVF, while severe adhesions may lower success. Nevertheless, the combination of hysteroscopy, hormonal therapy, and IVF has yielded satisfactory results in many patients.
Use of a Surrogate Uterus (Surrogacy)
When the patient’s uterus is severely damaged and the endometrium cannot thicken even after multiple surgeries or hormonal treatments, surrogacy may be recommended.
The embryo, created from the genetic parents’ eggs and sperm, develops in another woman’s uterus.
This approach is especially effective in extensive adhesions or complete destruction of the uterine cavity.
Post-IVF Care in Patients with Uterine Adhesions
– Regular use of hormonal medications (estrogen and progesterone) to support the endometrium and implantation
– Avoiding stress and heavy physical activity during the first weeks after transfer
– Follow-up with ultrasound and βhCG tests as advised by the doctor
– In cases with a history of severe adhesions, preventive treatments may be planned to reduce recurrence
Many women who experienced infertility due to uterine adhesions have achieved successful pregnancies with modern treatments combining hysteroscopy and IVF. Even in severe cases, surrogacy allows for having a genetically related child. The key is accurate diagnosis, step-by-step treatment, and consistent follow-up to achieve the best outcome for each patient.
Clinical cases
Case 1: Amenorrhea after D&C
A 30-year-old woman noticed her periods nearly stopped after a miscarriage and D&C. Imaging and hysteroscopy revealed severe adhesions. After surgical hysteroscopy, her periods returned within months.
Key point: Sudden absence of menstruation after D&C requires prompt evaluation.
Case 2: Long-standing infertility
A 35-year-old woman had tried to conceive for several years with normal ovarian and tubal function. Hysteroscopy showed extensive intrauterine adhesions. After surgery and hormonal therapy, she conceived and delivered a healthy baby.
Key point: Adhesions can be a hidden cause of infertility.
Case 3: Recurrent miscarriage
A 28-year-old woman had three consecutive miscarriages. Hysteroscopy revealed intrauterine adhesions impairing implantation. Surgical removal restored uterine function, and she carried her next pregnancy to term.
Key point: Repeated unexplained miscarriages warrant uterine evaluation for adhesions.
Conclusion
Uterine adhesions (Asherman’s syndrome) are a relatively common but treatable condition, often arising after D&C, surgery, or infection. They can cause irregular menstruation, infertility, or recurrent miscarriage. With timely diagnosis and surgical treatment using hysteroscopy, many women can regain normal uterine function and achieve successful pregnancy.
References

If your periods stopped or you have infertility after curettage or surgery?
Fill out the consultation form now and our assistant will contact you shortly.
 FAQ
FAQ
No comments have been posted.
Your email address will not be published. Required fields are marked *




