
Oligomenorrhea (Infrequent Periods): Causes, Diagnosis, and Management
Introduction
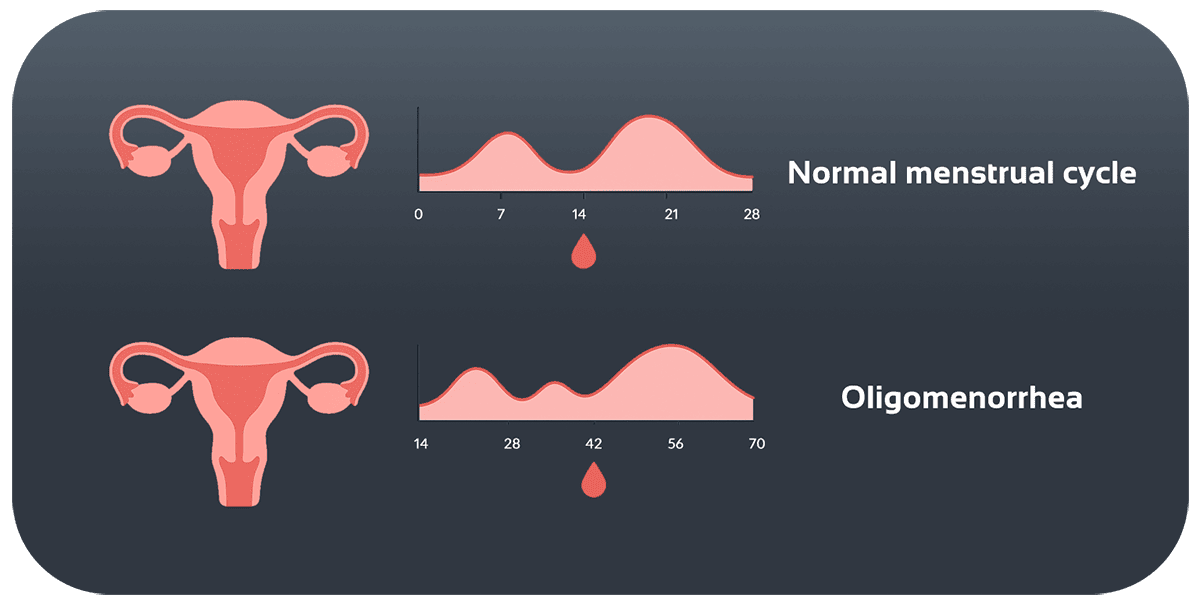
Oligomenorrhea refers to menstrual cycles that last longer than 35 days. It can be caused by irregular ovulation, hormonal fluctuations, thyroid disorders, or even high stress levels. Irregular periods often raise concerns about fertility and hormonal balance. Understanding the mechanisms and treatment options is key to maintaining women’s health and preventing long-term complications.
Types of Oligomenorrhea
-
Transient Oligomenorrhea
- Happens after temporary lifestyle changes like job stress, long travel, or sudden weight changes
- Cycles usually return to normal once conditions stabilize
-
Chronic Oligomenorrhea
- Persists for more than three consecutive cycles without spontaneous recovery
- Requires medical evaluation to identify underlying causes
Causes and Mechanisms
-
Hormonal Disorders of the Hypothalamus–Pituitary–Ovary Axis
- Reduced GnRH release due to chronic stress or hypothalamic dysfunction
- Lower LH and FSH levels, leading to incomplete or absent ovulation
-
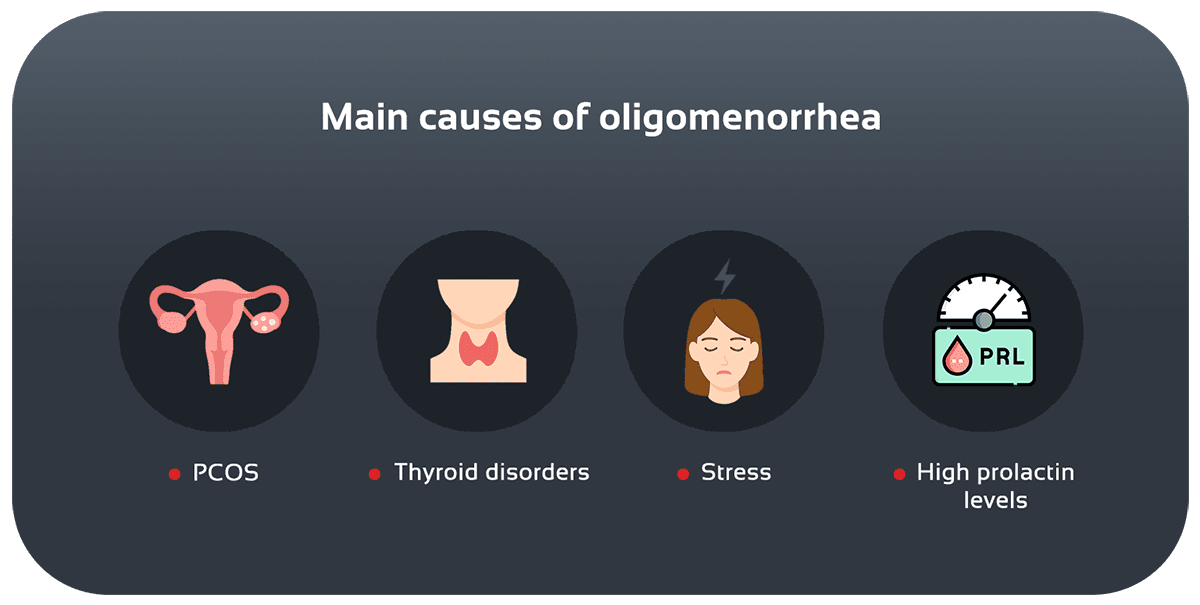
Polycystic Ovary Syndrome (PCOS)
- Insulin resistance and hyperandrogenism with multiple ovarian cysts
- Causes prolonged cycles and irregular bleeding
-
Thyroid Disorders
- Hypothyroidism: Increased TRH and prolactin levels, inhibiting ovulation
- Hyperthyroidism: Hormonal fluctuations and high metabolism affecting the pituitary axis
-
Hyperprolactinemia
- Small pituitary tumors (adenomas) or certain medications raise prolactin, blocking ovulation
-
Lifestyle and Environmental Factors
- Severe weight loss (BMI < 18.5) or obesity (BMI > 30)
- Excessive exercise without enough calorie intake
- High physical or emotional stress, including chronic illnesses
Clinical Features and Complications
- Irregular or long cycles: delays of 4–6 weeks or more
- Infertility or reduced fertility due to failed or incomplete ovulation
- Signs of androgen excess: acne, unwanted hair growth
- Irregular bleeding or spotting between cycles
- Fatigue, depression, mood swings caused by hormonal imbalance
Long-term risks include osteoporosis, early perimenopause, and cardiovascular disease.
Diagnosis
- Cycle Tracking: Using apps or calendars for at least three months
- Hormone Tests: FSH, LH, TSH, prolactin, testosterone, androgens
- Insulin Resistance Testing: Glucose tolerance test (GTT) for PCOS
- Transvaginal Ultrasound: To assess ovarian size, cysts, and endometrial thickness
- Pituitary MRI: If prolactin is high or tumor symptoms are suspected
Treatment and Management
Medication Options
- Combined oral contraceptives: Restore estrogen–progesterone balance and regular cycles
- Metformin: Improves insulin resistance in PCOS and helps ovulation
- Cabergoline/Bromocriptine: Lowers prolactin in hyperprolactinemia
Lifestyle Modifications
- Achieve and maintain a healthy BMI through balanced diet and exercise
- Stress management with yoga, meditation, or deep breathing
- Moderate-intensity exercise such as walking, swimming, cycling
Specialist Interventions
- Pituitary surgery: For adenomas unresponsive to medication
- Surgical management of rare ovarian or uterine structural abnormalities
Related Conditions
- PCOS: The most common cause of chronic oligomenorrhea
- Hyperprolactinemia: Often linked with mood or sleep issues
- Thyroid disorders: Especially hypothyroidism
Case Examples
- A 27-year-old woman with PCOS saw her cycle length improve from 60 days to 28–35 days after three months of metformin and dietary changes.
- A 34-year-old woman with a pituitary adenoma and high prolactin achieved four consecutive regular periods after bromocriptine therapy and MRI monitoring.
Prevention and Follow-Up
- Use a cycle calendar or app for accurate tracking
- Annual hormone testing to monitor balance
- Maintain a healthy weight and lifestyle
- Seek medical advice if periods are delayed for more than 6 weeks without an obvious reason
Conclusion
Oligomenorrhea is linked to multiple hormonal, endocrine, and lifestyle factors. With early diagnosis, proper treatment, and regular monitoring, cycles can often return to normal, preserving reproductive health. If you experience irregular or delayed periods, consult a gynecologist or endocrinologist.
References
- (2023). Oligomenorrhea: Etiology and management.
- (2015). Practice Bulletin No. 136: Management of Abnormal Uterine Bleeding.
- Endocrine Society. (2018). Clinical Practice Guidelines on Reproductive Endocrinology.

Take irregular periods seriously; your solution is here.
Fill out the consultation form now and our assistant will contact you shortly.
 FAQ
FAQ
No comments have been posted.
Your email address will not be published. Required fields are marked *




