
Placental Abnormalities | Placenta Previa and Placental Abruption
Introduction
The placenta is a vital organ in pregnancy, delivering oxygen and nutrients from mother to fetus and removing fetal waste. Any disruption in its position or function can seriously threaten the health of both mother and baby. Two of the most important placental disorders are placenta previa and placental abruption. Each can cause significant bleeding during pregnancy and, without timely diagnosis and management, may increase the risk of maternal or fetal death.
Section One: Placenta Previa
Definition
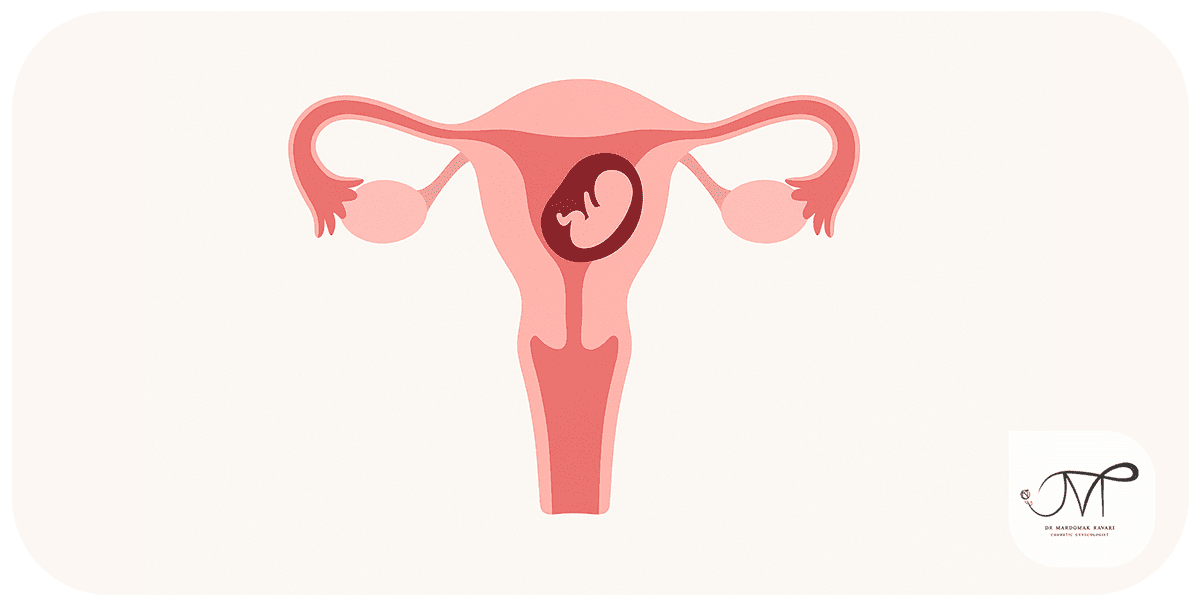
Placenta previa occurs when the placenta implants in the lower uterine segment and lies partially or completely over the cervical os instead of the upper or mid-uterus. This abnormal location can block the birth canal and raises the risk of significant bleeding, especially in the third trimester.
Normally, the placenta forms in the upper uterus, leaving room for fetal growth and an open path for delivery. In placenta previa, scarring or changes in the uterine lining shift implantation lower down. The condition is often detected by ultrasound in the first or second trimester; many cases resolve as the uterus grows and the placental edge “migrates.” If previa persists late in pregnancy, cesarean delivery is usually recommended to prevent hemorrhage.
Types
- Complete placenta previa: the placenta entirely covers the internal cervical os.
- Partial placenta previa: the placenta covers part of the os.
- Marginal placenta previa: the placental edge reaches the os but does not fully cover it.
Likely causes
– Uterine scarring: prior cesarean birth, myomectomy, or curettage can create scar tissue that alters implantation.
– Uterine structural anomalies: bicornuate uterus, septate uterus, or other congenital variants.
– Idiopathic low implantation: sometimes the placenta implants low without identifiable scarring; early cases may resolve as pregnancy advances.
– Uterine blood flow variation: reduced perfusion to upper segments may favor implantation in better-perfused lower segments.
Risk factors
- High parity and multiple prior deliveries
- History of placenta previa in a previous pregnancy
- Previous cesarean births, especially multiple
- Maternal age over 35 years
- Multiple gestation
- Cigarette smoking or substance use
- Conception via assisted reproductive technology such as IVF
- Short interpregnancy interval
Clinical features
- Painless vaginal bleeding, typically in the second or third trimester
- Sometimes mild contractions or none at all
- Fetal status usually reassuring unless bleeding is heavy
Diagnosis
– Transvaginal or transabdominal ultrasound to define placental location
– Fetal surveillance in higher-risk pregnancies using NST or BPP
Management
Treatment depends on gestational age, bleeding severity, placental position relative to the cervix, and maternal–fetal status.
-
Expectant management
Used when bleeding is absent or mild, the fetus is preterm, and monitoring is feasible.
- Activity modification or bed rest as advised
- Pelvic rest and abstinence from intercourse
- Serial clinical and ultrasound follow up
- Education on warning signs such as heavy bleeding, contractions, or abdominal pain requiring urgent evaluation
- Corticosteroids between approximately 24 and 34 weeks if preterm delivery is a concern to promote fetal lung maturity
-
Delivery planning
- For persistent complete previa, planned cesarean at about 36 to 37 weeks before labor begins
- Intraoperative preparedness for hemorrhage, including blood products
- Neonatal team present, particularly if preterm birth is anticipated
-
Emergency management
Immediate cesarean delivery if bleeding is uncontrolled or life-threatening, regardless of gestational age, to protect maternal and fetal lives
-
After diagnosis
- Carry a high-risk pregnancy card or documentation
- Psychological support due to stress and potential hospitalizations
- Iron supplementation and nutrition optimization to mitigate anemia
Potential complications if untreated
- Severe hemorrhage and shock
- Maternal or fetal death
- Preterm birth
- Fetal growth concerns due to impaired placental function
Section Two: Placental Abruption
Definition
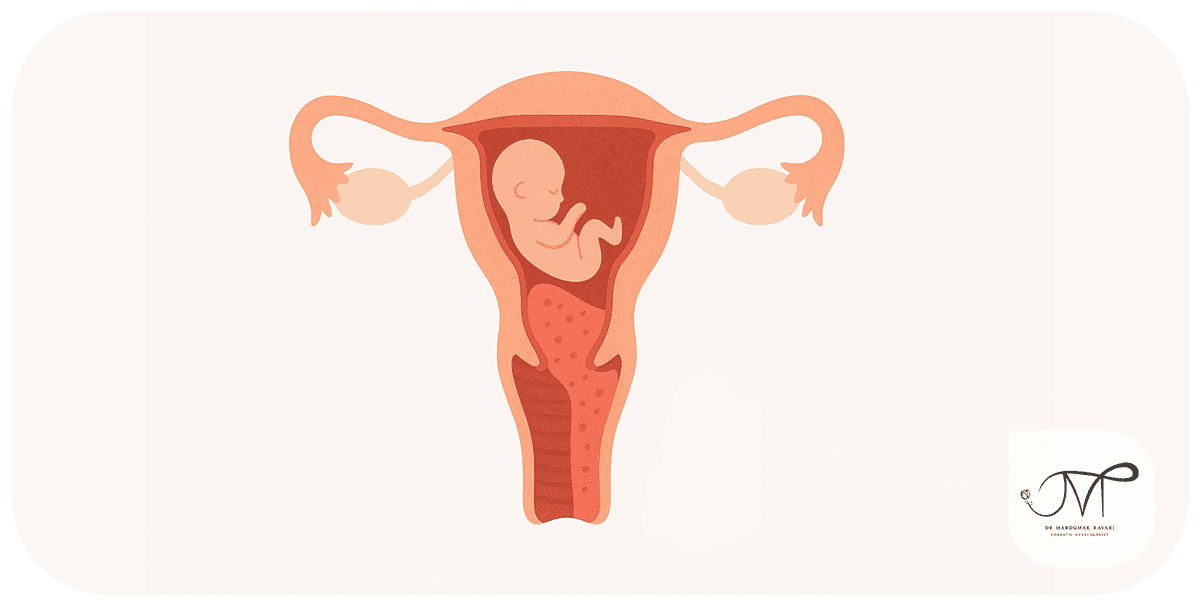
Placental abruption is the premature separation of the placenta from the uterine wall before delivery. It usually occurs in the third trimester but can happen any time after 20 weeks. Because the placenta is the fetus’s sole source of oxygen and nutrients, separation disrupts this exchange and can rapidly endanger the fetus and mother.
Severity relates to the extent of detachment:
– Partial abruption: a segment separates; with close monitoring, pregnancy may continue in selected cases.
– Complete abruption: total separation, causing cessation of fetal blood flow and a life-threatening emergency.
Pathophysiology involves bleeding at the placental–uterine interface, forming a hematoma that shears the placenta away, either gradually or abruptly.
Why it matters
– Even brief interruptions in placental perfusion can cause fetal hypoxia, brain injury, or death.
– Maternal hemorrhage can lead to shock, organ failure, or death.
Causes and risk factors
Possible causes
- Abdominal trauma
– Motor vehicle crash, fall, or direct blow can rupture placental vessels.
- Uterine or placental problems
– Structural uterine issues or surgical scars after cesarean or myomectomy may weaken attachment sites.
- Premature rupture of membranes
– Loss of amniotic fluid reduces intrauterine volume and may trigger separation.
- Coagulation disorders
– Conditions affecting clotting increase bleeding risk at the interface.
- Intrauterine infections
– Inflammation weakens placental attachment.
Major risk factors
- Hypertension or preeclampsia
– The most important risk factor; vascular damage reduces placental perfusion.
- Prior placental abruption
– Recurrence risk is elevated in subsequent pregnancies.
- Smoking or cocaine use
– Vasoconstriction and reduced uteroplacental blood flow raise risk.
- Multiple gestation
– Greater uterine distension increases mechanical stress.
- Maternal age over 35 years
- Precipitate labor or hyperstimulation with strong contractions
- First or second trimester bleeding as a marker of placental vulnerability
Clinical features
- Vaginal bleeding, which may be concealed
- Abdominal or pelvic pain
- Firm, tender, or “board-like” uterus
- Decreased or absent fetal movements
- Maternal signs of shock such as hypotension and tachycardia
Diagnosis
- Clinical assessment and history
- Ultrasound, noting that sensitivity is limited and abruption can be missed
- Fetal well-being evaluation with NST or BPP
Management of placental abruption

Care is driven by severity of separation, gestational age, maternal stability, fetal status, and extent of bleeding.
-
Immediate evaluation and stabilization
– Check maternal vital signs and level of consciousness
– Continuous fetal heart rate monitoring
– Urgent laboratory tests including hemoglobin and coagulation profile
– Intravenous fluids and blood products as indicated
– Bed rest and observation to limit progression if appropriate
-
Decision making by severity
a) Mild and stable abruption
– Low-volume bleeding, reassuring fetal tracing, gestational age under about 34 weeks
– Hospital observation, blood pressure control, corticosteroids for fetal lungs if preterm delivery becomes necessary, and close maternal–fetal surveillance
b) Moderate or evolving abruption
– Increasing bleeding, maternal anemia, decreased fetal movement, or nonreassuring tracings
– Continued monitoring and readiness to deliver
– If gestational age is at or beyond about 34 weeks, delivery is often indicated. Vaginal birth may be considered if maternal–fetal status is stable; otherwise cesarean delivery is performed.
c) Severe, life-threatening abruption
– Heavy bleeding, persistent abdominal pain, maternal shock, or fetal distress
– Emergency cesarean if the fetus is viable
– If fetal demise has occurred, expedited vaginal delivery is generally safer for the mother than surgery
– Aggressive transfusion support and management of coagulopathy, including DIC, when present
-
Supportive measures
– Rigorous blood pressure control, especially with preeclampsia
– Fluids and vasopressors as needed in shock
– Multidisciplinary coordination among obstetrics, anesthesia, and neonatology
-
Postpartum care
– Inspect uterus and placenta to document abruption
– Monitor for postpartum hemorrhage
– Treat anemia with iron and transfusion as needed
– Provide psychological support given the traumatic nature of the event
-
Reducing recurrence risk in future pregnancies
– Optimal blood pressure management
– Strict avoidance of smoking and drug use
– Regular prenatal care with interval ultrasounds
– Enhanced surveillance for those with a prior abruption

Complications if untreated
– Fetal death from hypoxia
– Maternal shock and death
– Disseminated intravascular coagulation
– Uterine damage and long-term reproductive risks
Prevention strategies for placental disorders
– Meticulous blood pressure control during pregnancy
– Smoking and substance cessation
– Routine prenatal visits and recommended ultrasounds
– Avoiding high-risk activities that could cause abdominal trauma
– Managing chronic diseases before and during pregnancy
Clinical examples
- Placenta previa: A 36-year-old with two prior cesareans presented at 30 weeks with painless bleeding. Ultrasound confirmed complete previa. She was managed in hospital and underwent planned cesarean at 37 weeks.
- Placental abruption: A 28-year-old with hypertension presented at 34 weeks with severe abdominal pain. Evaluation showed extensive abruption and nonreassuring fetal status. Emergency cesarean was performed.
Conclusion
Placental disorders are among the most serious complications of pregnancy and can be life-threatening for mother and baby. Recognizing warning signs, seeking prompt medical care, and adhering to prenatal recommendations are essential to early diagnosis and effective management.
References

If you have bleeding or abdominal pain during pregnancy, see your doctor or go to the ER immediately!
Fill out the consultation form now and our assistant will contact you shortly.
 FAQ
FAQ
No comments have been posted.
Your email address will not be published. Required fields are marked *
Share:




